 , Mehmet Ali Astarcıoğlu 2
, Fahriye Vatansever Ağca 3
, Ahmet Seyda Yılmaz 4
, Gülşah Aktüre 5
, Ahmet Oğuz Aslan 6
, Flora Özkalaycı 7
, Bedri Caner Kaya 8
, Ümit Güray 9
, Utku Uluköksal 1
, Barış Şimşek 1
, Hüseyin Emre Kuloğlu 10
, Rabia Çoldur 11
, Furkan Karahan 12
, İbrahim Halil Tanboğa 13
, Mehmet Ali Astarcıoğlu 2
, Fahriye Vatansever Ağca 3
, Ahmet Seyda Yılmaz 4
, Gülşah Aktüre 5
, Ahmet Oğuz Aslan 6
, Flora Özkalaycı 7
, Bedri Caner Kaya 8
, Ümit Güray 9
, Utku Uluköksal 1
, Barış Şimşek 1
, Hüseyin Emre Kuloğlu 10
, Rabia Çoldur 11
, Furkan Karahan 12
, İbrahim Halil Tanboğa 13
2Department of Cardiology, Kütahya Health and Science University Evliya Celebi Training and Research Hospital, Kütahya, Türkiye
3Department of Cardiology, Bursa High Specialization Training and Research Hospital, Bursa, Türkiye
4Department of Cardiology, Recep Tayyip Erdoğan University Faculty of Medicine, Rize, Türkiye
5Department of Cardiology, Düzce University Training and Research Hospital, Düzce, Türkiye
6Department of Cardiology, Ahi Evren Thoracic and Cardiovascular Surgery Training and Research Hospital, Trabzon, Türkiye
7Department of Cardiology, Hisar Hospital Intercontinental, İstanbul, Türkiye
8Department of Cardiology, Şanlıurfa Mehmet Akif İnan Training and Research Hospital, Şanlıurfa, Türkiye
9Department of Cardiology, Ankara Bilkent City Hospital, Ankara, Türkiye
10Department of Cardiology, İnönü University Faculty of Medicine, Malatya, Türkiye
11Department of Cardiology, Van Yüzüncü Yıl University Faculty of Medicine, Van, Türkiye
12Department of Cardiology, Trakya University Faculty of Medicine, Edirne, Türkiye
13Department of Biostatistics, Nişantaşı University Faculty of Medicine, İstanbul, Türkiye
Abstract
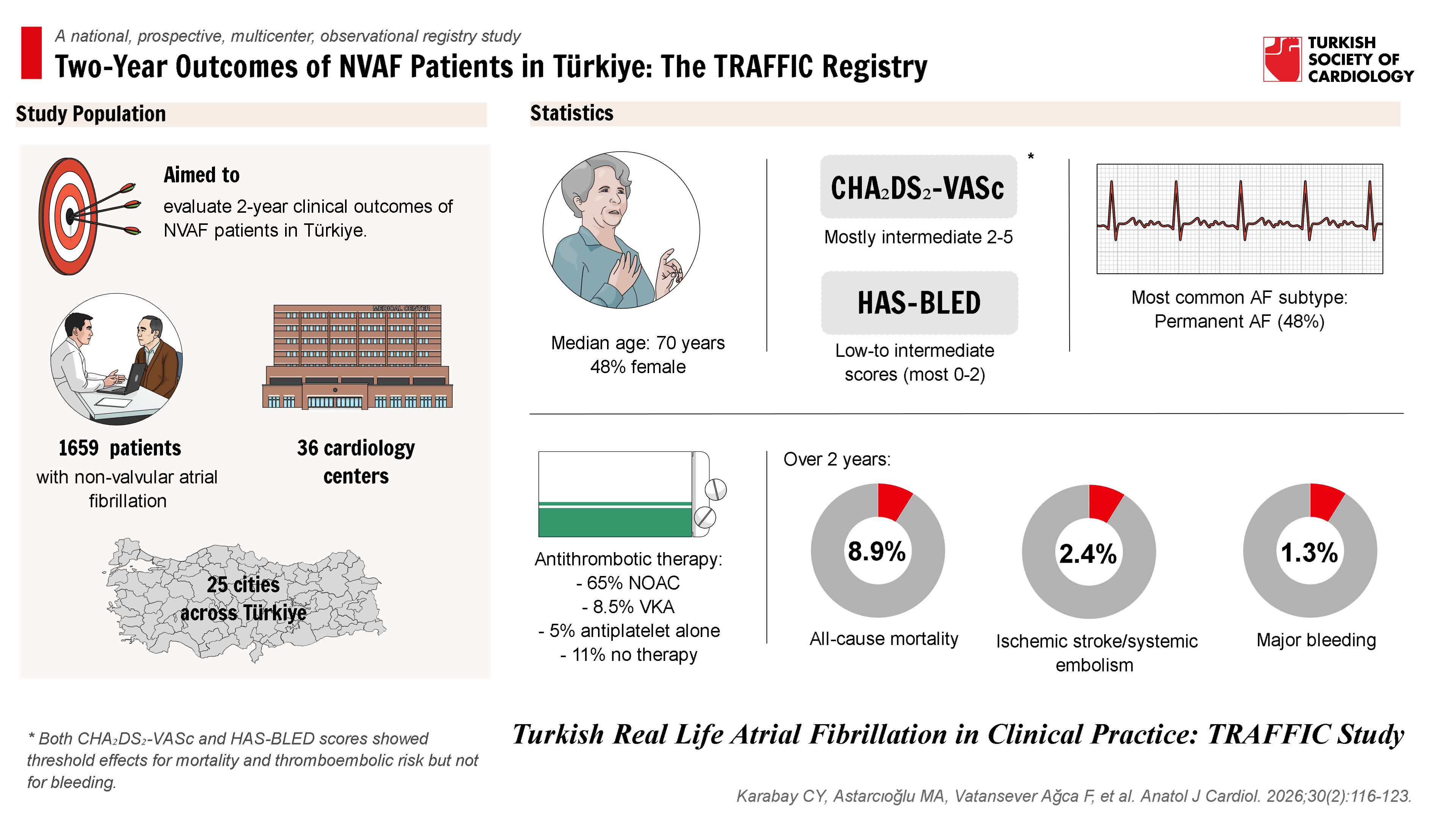
Background: Atrial fibrillation (AF) is a major public health issue associated with thromboembolism and mortality. Real-world data from Türkiye are limited despite expanding use of non-vitamin K antagonist oral anticoagulants (NOACs). The Turkish Real Life Atrial Fibrillation in Clinical Practice (TRAFFIC) study aimed to characterize the demographic features, risk profiles, treatment patterns, and 2-year clinical outcomes of patients with non-valvular AF (NVAF) in Türkiye.
Methods: TRAFFIC was a national, prospective, multicenter, observational registry enrolling 1659 NVAF patients from 36 centers with 6-monthly follow-up for 24 months. Baseline data included demographics, comorbidities, CHA₂DS₂-VASc, HAS-BLED, AF subtype, European Heart Rhythm Association (EHRA) score, and antithrombotic therapy. Outcomes were ischemic stroke/systemic embolism (SE), major bleeding, and all-cause mortality. Predictors of mortality were evaluated using adjusted Cox regression, and associations of risk scores were explored using univariate Cox models with restricted cubic splines.
Results: Median age was 70 years, 48% female, with intermediate CHA₂DS₂-VASc (most 2-5) and low-to-intermediate HAS-BLED scores (most 0-2). Permanent AF was the most common subtype (48%). Antithrombotic therapy largely reflected risk profiles, with NOACs being the dominant treatment (65%). Over 2 years, all-cause mortality was 8.9%, ischemic stroke/SE 2.4%, and major bleeding 1.3%. In adjusted analysis, age, congestive heart failure, and diabetes mellitus were independent predictors of mortality. Both CHA₂DS₂-VASc and HAS-BLED scores showed threshold effects for mortality and thromboembolic risk but not for bleeding.
Conclusion: TRAFFIC provides contemporary Turkish NVAF data, showing lower event rates than historical cohorts. Outcomes are comparable with international registries; persistent mortality burden highlights the need for AF care beyond anticoagulation.
Graphical Abstract
Highlights
- Contemporary real-world Turkish NVAF data from the TRAFFIC registry show NOACs as the predominant antithrombotic strategy and overall low 2-year event rates.
- Two-year outcomes were favorable (mortality 8.9%, ischemic stroke/SE 2.4%, major bleeding 1.3%) and broadly comparable to international registries.
- Mortality was independently associated with age, heart failure, and diabetes, highlighting residual risk and the need for comprehensive AF care beyond anticoagulation.
Introduction
Atrial fibrillation (AF), the most common sustained cardiac arrhythmia in the general population, imposes a significant global public health burden.1 Beyond substantially increasing the risk of thromboembolic events, particularly ischemic stroke, AF is associated with heart failure, impaired quality of life, and increased mortality.2,
Previous important data regarding the prevalence, incidence, and outcomes of AF in Türkiye were derived from the TEKHARF study, which included follow-up data until 2006-2007.8 However, since then, developments in diagnostic and therapeutic approaches and the widespread introduction of NOACs have necessitated the collection of contemporary real-world data. At the international level, large prospective registry studies like GARFIELD-AF have played a crucial role in elucidating the characteristics, treatment patterns, and clinical outcomes of AF patients in real-world settings.9 These registries have demonstrated current practice variations and levels of guideline adherence across different geographies and care settings. Data from GARFIELD-AF, for instance, highlighted that the highest event rates (stroke, bleeding, mortality) occur in the early period after diagnosis and that mortality is a more frequent outcome than stroke.10
In this context, there was a need for a national, prospective, real-world registry to evaluate the current demographic characteristics, risk profiles, treatment patterns, and clinical outcomes of the contemporary AF patient population in Türkiye, reflecting the impact of evolving diagnostic and therapeutic approaches. The TRAFFIC (Turkish Real Life Atrial Fibrillation in Clinical Practice) study aims to prospectively examine the current management and 2-year clinical outcomes of NVAF patients across Türkiye. This study seeks to reveal the current state of AF management practice in Türkiye, provide a benchmark for comparison with international real-world data, and establish a foundation for future clinical practice and research.
Methods
Study Design and Participants
The TRAFFIC study is a national, prospective, multicenter, observational registry conducted across Türkiye. The study protocol was reviewed and approved by an independent ethics committee and was conducted in accordance with the principles of the Declaration of Helsinki.11 Written informed consent was obtained from all participating patients.12
The study population comprised consecutive patients diagnosed with non-valvular atrial fibrillation (NVAF) aged 18 years and older, enrolled from 36 cardiology centers in 25 different cities across Türkiye between July 2020 and October 2022. The diagnosis of NVAF was confirmed by ECG or 24-hour Holter recording at the time of enrollment or within the preceding 6 weeks, or included patients with a medical history of AF who were currently receiving treatment. Patients with valvular AF (rheumatic mitral stenosis, mechanical or bioprosthetic heart valves), AF due to transient or reversible causes, and those with a life expectancy of less than 6 months that would preclude study participation were excluded. Only patients who attended at least the 6-month follow-up visit, thus allowing outcome assessment, were included in the final analysis. The selection of centers aimed to represent different geographical regions of Türkiye (according to the NUTS-2 classification).13
Data Collection
Patient data were collected prospectively through face-to-face clinical visits at baseline and subsequently at 6, 12, 18, and 24 months. During the data collection process, patients’ demographic information, medical history (including comorbidities and risk factors), vital signs, AF symptoms (EHRA score), ECG and echocardiographic findings, CHA₂DS₂-VASc and HAS-BLED risk scores, applied interventional treatments (cardioversion, catheter ablation, etc.), and current antithrombotic and antiarrhythmic medications were recorded. Event data (ischemic stroke, systemic embolism [SE], major bleeding, all-cause mortality, cardiovascular death, non-cardiovascular death, and hospitalizations) were ascertained during follow-up visits and confirmed from medical records. Data were entered into web-based electronic case report forms (eCRFs).
Definitions and Endpoints
The definitions used in the study were based on standard clinical guidelines. CHA₂DS₂-VASc and HAS-BLED scores were used to assess patients’ thromboembolic and bleeding risks, respectively.14,
Statistical Analysis
Baseline characteristics and demographic data are presented using descriptive statistics. Continuous variables are expressed as median and interquartile range (IQR), while categorical variables are presented as counts and percentages.
Event rates for ischemic stroke/SE, major bleeding, and all-cause mortality over the 2-year follow-up period were calculated. Independent predictors for all-cause mortality were assessed using an adjusted Cox proportional hazards regression model. Factors considered in this model included age, congestive heart failure, diabetes mellitus, AF subtype (paroxysmal, persistent, newly diagnosed, long-standing persistent, permanent), and baseline antithrombotic treatment strategy (NOAC, VKA, antiplatelet alone, no therapy). Analysis results are presented with hazard ratios (HRs), 95% CIs, and statistical significance levels (
Results
From July 2020 to October 2022, a total of 1659 patients were prospectively enrolled with NVAF across 36 centers in 25 Turkish cities. However, in this study, only patients who completed at least the 6-month follow-up visit, enabling outcome assessment, were included in the analysis, resulting in a final cohort of 1442 patients. At baseline, the current cohort of 1659 patients (median age 70 years, IQR 62-77; 48% female) exhibited a wide spectrum of thromboembolic and bleeding risk, AF phenotypes, and symptom burden. CHA₂DS₂-VASc scores clustered between 2 and 5 (≈75% of patients), while HAS-BLED scores were predominantly 0-2 (≈86%). Across both risk scales, NOACs were the dominant therapy (~60%-80%), with VKAs and antiplatelets used infrequently and untreated rates dropping below 5% at higher CHA₂DS₂-VASc levels (
During the 2-year follow-up, 126 patients (8.9%) died—17 (1.2%) from cardiovascular causes, 51 (3.6%) from non-cardiovascular causes, and 58 (4.1%) of undetermined etiology. Ischemic stroke occurred in 26 (1.8%), Ischemic stroke/SE in 34 (2.4%), and major bleeding in 18 (1.3%). In the adjusted Cox model, each interquartile‐range increase in age (from the 25th to the 75th percentile, 62.3-77.3 years) was associated with a more than 2-fold higher hazard of death (HR 2.33; 95% CI 1.74-3.13;
To explore unadjusted associations, it was found that both CHA₂DS₂-VASc and HAS-BLED scores exhibit threshold effects for mortality and thromboembolic risk, but not for bleeding. In the upper row (panels A–C), CHA₂DS₂-VASc points below approximately 2 carry minimal change in hazard, whereas an interquartile‐range increase in score (from the 25th to the 75th percentile) corresponds to a 36% higher unadjusted risk of all‐cause death (HR 1.36; 95% CI 1.08-1.71;
Discussion
This prospective nationwide cohort study provides contemporary data on the demographic characteristics, risk profiles, treatment patterns, and clinical outcomes of 1659 Turkish patients with NVAF enrolled between July 2020 and October 2022. The current findings reflect a broad spectrum of thromboembolic and bleeding risks, diverse AF phenotypes, and varying symptom burdens, aligning closely with international registries while highlighting distinct regional trends.17-
Our cohort exhibited intermediate event rates compared with historical national data and recent international registries.8,
Similarly, the all-cause mortality rate (~6-7% annually) observed in this cohort occupies an intermediate position—lower than historical Turkish data (TRAF, 11.5%) but higher compared to recent European data (EORP-AF, 5.2%).20,
Regarding major bleeding events (~2% per year), these findings are broadly similar to both historical national (TRAF, 2.0%) and recent European data (EORP-AF, 2.3%), indicating that modern anticoagulation strategies in Türkiye effectively manage bleeding risks at acceptable levels.20,
Treatment patterns in the current cohort strongly reflected current European Society of Cardiology (ESC) guidelines, with widespread anticoagulant use among high-risk patients, predominantly NOACs.14 This represents a significant shift from earlier practices dominated by VKAs, underscoring an evolution toward safer and more effective therapies. Compared to EORP-AF (2017-2018), where NOAC use was 33%, this study reported a much higher rate (65%), highlighting improved guideline adherence and increased NOAC availability in Türkiye.23 This transition likely contributed to the observed reduction in thromboembolic events. Furthermore, the current analysis reaffirmed the prognostic importance of AF subtypes. Persistent and permanent AF were associated with higher morbidity and mortality compared to paroxysmal AF, aligning with findings from EORP-AF and other international registries.24-
Clinical implications of this study highlight the tangible benefits of modern NVAF management strategies, particularly widespread anticoagulation with NOACs, in reducing stroke risk. However, the notable residual annual mortality (~6%-7%) emphasizes that comprehensive AF care must extend beyond anticoagulation to include rigorous risk-factor modification, symptom management, and targeted rhythm or rate control interventions.
Strengths of this study include its large sample size, nationwide scope covering diverse geographic regions, and a rigorous prospective design with a comprehensive data collection strategy over a substantial 2-year follow-up period. These factors enhance the generalizability and relevance of these findings. Nevertheless, the current study has several limitations. First, its observational nature precludes definitive causal conclusions. Additionally, the 2-year follow-up, while informative, may not fully capture long-term outcomes. Potential biases arising from center selection and variability in data adjudication could influence results, limiting generalizability. Detailed socio-economic and educational factors influencing treatment adherence and outcomes were not extensively captured. These considerations underline the importance of cautious interpretation and the need for continued, longer-term research.
Conclusion
In conclusion, the large-scale, multicenter Turkish cohort demonstrates significantly improved outcomes compared to historical national data, aligning closely with international registries, driven predominantly by increased NOAC utilization and guideline-concordant practices. However, residual morbidity and mortality highlight the need for continued emphasis on comprehensive AF management strategies. These findings provide a valuable benchmark for Türkiye and contribute to global efforts toward evidence-based NVAF care optimization.
Footnotes
The authors gratefully acknowledge the unconditional support of the Turkish Society of Cardiology, as well as the partial support provided by Pfizer Inc.
References
- Chugh SS, Havmoeller R, Narayanan K. Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 Study. Circulation. 2014;129(8):837-847. https://doi.org/10.1161/CIRCULATIONAHA.113.005119
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98(10):946-952. https://doi.org/10.1161/01.cir.98.10.946
- Ko D, Chung MK, Evans PT, Benjamin EJ, Helm RH. Atrial fibrillation: a review. JAMA. 2025;333(4):329-342. https://doi.org/10.1001/jama.2024.22451
- Fauchier L, Villejoubert O, Clementy N. Causes of death and influencing factors in patients with atrial fibrillation. Am J Med. 2016;129(12):1278-1287. https://doi.org/10.1016/j.amjmed.2016.06.045
- Marijon E, Le Heuzey JY, Connolly S. Causes of death and influencing factors in patients with atrial fibrillation: a competing-risk analysis from the randomized evaluation of long-term anticoagulant therapy study. Circulation. 2013;128(20):2192-2201. https://doi.org/10.1161/CIRCULATIONAHA.112.000491
- Lee E, Choi EK, Han KD. Mortality and causes of death in patients with atrial fibrillation: a nationwide population-based study. PLoS One. 2018;13(12):e0209687-. https://doi.org/10.1371/journal.pone.0209687
- Freedman B, Potpara TS, Lip GYH. Stroke prevention in atrial fibrillation. Lancet. 2016;388(10046):806-817. https://doi.org/10.1016/S0140-6736(16)31257-0
- Uyarel H, Onat A, Yüksel H, Can G, Ordu S, Dursunoğlu D. Incidence, prevalence, and mortality estimates for chronic atrial fibrillation in Turkish adults. Turk Kardiyol Dern Ars. 2008;36(4):214-222.
- Bassand JP, Accetta G, Camm AJ. Two-year outcomes of patients with newly diagnosed atrial fibrillation: results from GARFIELD-AF. Eur Heart J. 2016;37(38):2882-2889. https://doi.org/10.1093/eurheartj/ehw233
- Bassand JP, Virdone S, Goldhaber SZ. Early risks of death, stroke/systemic embolism, and major bleeding in patients with newly diagnosed atrial fibrillation. Circulation. 2019;139(6):787-798. https://doi.org/10.1161/CIRCULATIONAHA.118.035012
- . World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. https://doi.org/10.1001/jama.2013.281053
- Karabay CY, Taşolar H, Ülgen Kunak A. Turkish real life atrial fibrillation in clinical practice: TRAFFIC study. Anatol J Cardiol. 2024;28(2):87-93. https://doi.org/10.14744/AnatolJCardiol.2023.3616
- . . Statistical Regions Level 2 in turkey. 2016;():-. https://ec.europa.eu/eurostat/documents/345175/7773495/TR.pdf
- Hindricks G, Potpara T, Dagres N. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373-498. https://doi.org/10.1093/eurheartj/ehaa612
- Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJGM, Lip GYH. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the euro Heart Survey. Chest. 2010;138(5):1093-1100. https://doi.org/10.1378/chest.10-0134
- Fasulo MR, Biguzzi E, Abbattista M. The ISTH bleeding assessment tool and the risk of future bleeding. J Thromb Haemost. 2018;16(1):125-130. https://doi.org/10.1111/jth.13883
- Romiti GF, Corica B, Mei DA. Patterns of comorbidities in patients with atrial fibrillation and impact on management and long-term prognosis: an analysis from the prospective global GLORIA-AF Registry. BMC Med. 2024;22(1):151-. https://doi.org/10.1186/s12916-024-03373-4
- Beier L, Lu S, França LR. Evolution of antithrombotic therapy for patients with atrial fibrillation: the prospective global GLORIA-AF registry program. PLoS One. 2022;17(10):e0274237-. https://doi.org/10.1371/journal.pone.0274237
- Bakhai A, Darius H, De Caterina R. Characteristics and outcomes of atrial fibrillation patients with or without specific symptoms: results from the PREFER in AF registry. Eur Heart J Qual Care Clin Outcomes. 2016;2(4):299-305. https://doi.org/10.1093/ehjqcco/qcw031
- Yavuz B, Ata N, Oto E. Demographics, treatment and outcomes of atrial fibrillation in a developing country: the population-based Turkish atrial fibrillation (TRAF) cohort. Europace. 2017;19(5):734-740. https://doi.org/10.1093/europace/euw385
- Lip GYH, Laroche C, Ioachim PM. Prognosis and treatment of atrial fibrillation patients by European cardiologists: one year follow-up of the EURObservational research programme-atrial fibrillation general registry pilot phase (EORP-AF Pilot registry). Eur Heart J. 2014;35(47):3365-3376. https://doi.org/10.1093/eurheartj/ehu374
- Proietti M, Romiti GF, Vitolo M, Potpara TS, Boriani G, Lip GYH. Comparison of HAS-BLED and ORBIT bleeding risk scores in atrial fibrillation patients treated with non-vitamin K antagonist oral anticoagulants: a report from the ESC-EHRA EORP-AF General Long-Term Registry. Eur Heart J Qual Care Clin Outcomes. 2022;8(7):778-786. https://doi.org/10.1093/ehjqcco/qcab069
- Boriani G, Proietti M, Laroche C. Changes to oral anticoagulant therapy and risk of death over a 3-year follow-up of a contemporary cohort of European patients with atrial fibrillation final report of the EURObservational research programme on atrial fibrillation (EORP-AF) pilot general registry. Int J Cardiol. 2018;271():68-74. https://doi.org/10.1016/j.ijcard.2018.05.034
- Apiyasawat S, Kornbongkotmas S, Chichareon P, Krittayaphong R. Mortality risk and temporal patterns of atrial fibrillation in the nationwide registry. J Arrhythm. 2021;37(6):1434-1442. https://doi.org/10.1002/joa3.12643
- Blum S, Aeschbacher S, Coslovsky M. Long-term risk of adverse outcomes according to atrial fibrillation type. Sci Rep. 2022;12(1):2208-. https://doi.org/10.1038/s41598-022-05688-9
- Boriani G, Laroche C, Diemberger I. ‘Real-world’ management and outcomes of patients with paroxysmal vs. non-paroxysmal atrial fibrillation in Europe: the EURObservational research programme-atrial fibrillation (EORP-AF) general pilot registry. Europace. 2016;18(5):648-657. https://doi.org/10.1093/europace/euv390